
Achondroplasia is a genetic disorder that affects bone growth and results in short stature. It is caused by a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene, which is located on chromosome 4p16.3[1].
This mutation leads to abnormal cartilage formation and impaired bone growth, resulting in the characteristic features of achondroplasia[2].
It is the most common form of dwarfism, affecting approximately 1 in 15,000 to 40,000 live births[1].
Etiology of Achondroplasia
It is caused by a mutation in the FGFR3 gene, which encodes a protein that is involved in the regulation of bone growth[1]. This mutation leads to abnormal cartilage formation and impaired bone growth, resulting in the characteristic features of achondroplasia[2].
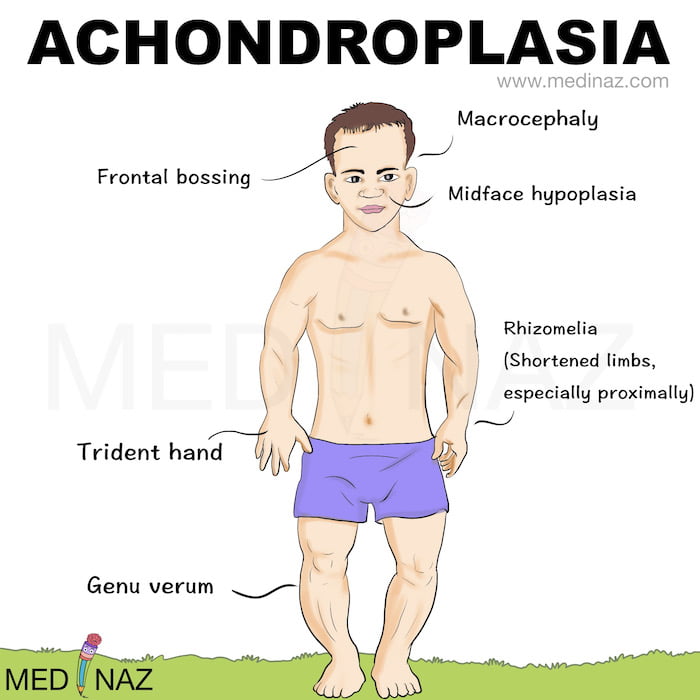
Achondroplasia Clinical Presentation
It is characterized by rhizomelic shortening of the limbs, which means that the upper arms and thighs are more affected than the forearms and lower legs. Here is a list of some of the clinical features of achondroplasia:
- Shortened arms and legs, with the upper arms and thighs more affected than the forearms and lower legs
- Large head size with a prominent forehead
- Flat nose
- Short hands and feet
- Large separation between third and fourth fingers
- Maximum height of 4 feet
- Bowed legs
- Pronounced and permanent sway of the lower back (lordosis)
- Abnormal front-to-back curvature of the spine (kyphosis)
- Back and leg pain
- Breathing problems (apnea)
- Obesity
- Recurring ear infections
- Excess fluid on the brain (hydrocephalus)
Pathogenesis:
- Achondroplasia is caused by autosomal dominant mutations in fibroblast growth factor receptor 3 (FGFR3).
- FGFR3 is expressed in chondrocytes and mature osteoblasts where it functions to regulate bone growth.
- Increased FGFR3 signaling suppresses proliferation and maturation of growth plate chondrocytes resulting in decreased growth plate size, reduced trabecular bone volume, and resulting decreased bone elongation.
- Current therapeutic strategies have focused on reducing signals emanating from FGFR3, and counteracting signal transduction pathways downstream of FGFR3 holds promise.
- Michelin tire baby syndrome (MTBS) is a rare genodermatosis characterized by generalized excessive skin folds and may or may not be associated with chromosomal abnormalities.
- A rare association of Michelin tire baby syndrome with achondroplasia has been reported in India and Yemen.
- Vozoritide is the first drug that has an effect on the pathogenesis of impaired enchondral growth in achondroplasia and has shown effectiveness in clinical trials.
Achondroplasia Radiology:
Radiological features of achondroplasia are important for diagnosis and management of the condition. Here are some radiological features of achondroplasia based on the search results:
A small foramen magnum: This is a common radiological feature of achondroplasia and is due to the narrowing of the base of the skull[3][4].
Short pedicles: Pedicles are the bony projections that connect the vertebral body to the facet joints. In achondroplasia, the pedicles are shorter than normal, which can lead to spinal stenosis[3].
Narrow spinal canal: The spinal canal is the space within the spinal column that contains the spinal cord. In achondroplasia, the spinal canal is narrower than normal, which can lead to spinal cord compression[3][4].
Flattened vertebral bodies: The vertebral bodies in achondroplasia are often flattened and have a rectangular shape[3].
Shortened long bones: The long bones in the arms and legs are disproportionately short in achondroplasia, which is known as rhizomelic shortening[3][5].
Bowing of the long bones: The long bones in the arms and legs may also be bowed in achondroplasia[4].
Prominent forehead: The forehead in achondroplasia is often prominent due to the underdevelopment of the mid face[3].
Depressed nasal bridge: The nasal bridge in achondroplasia is often depressed, which can contribute to the characteristic facial appearance[6].
Management:
Management may include monitoring for complications such as spinal stenosis, sleep apnea, and obesity.
Surgery may be necessary to relieve spinal cord compression.
Growth hormone therapy may be used to increase height, but it is not a cure for achondroplasia[1].
Clinical management of achondroplasia should be individualized based on the patient’s specific needs and should involve a multidisciplinary team of healthcare professionals[2].
Clinical Points to Remember
- It is a genetic disorder that affects bone growth and results in short stature.
- It is caused by a mutation in the FGFR3 gene, which encodes a protein that is involved in the regulation of bone growth.
- The phenotypical characteristics of achondroplasia include short stature, disproportionately short limbs, and a relatively large head.
- Radiological features of achondroplasia include a small foramen magnum, short pedicles, and a narrow spinal canal.
- Management of achondroplasia may include monitoring for complications such as spinal stenosis, sleep apnea, and obesity.
- Surgery may be necessary to relieve spinal cord compression.
- Growth hormone therapy may be used to increase height, but it is not a cure for achondroplasia.
- Clinical management of achondroplasia should be individualized based on the patient’s specific needs and should involve a multidisciplinary team of healthcare professionals.
Citations:
[1] https://pubmed.ncbi.nlm.nih.gov/29185944/ [2]https://www.semanticscholar.org/paper/115c356ac6113cab88d4827b9f866b53d4819fba [3] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7654452/ [4] https://pubmed.ncbi.nlm.nih.gov/29185944/ [5] https://pubmed.ncbi.nlm.nih.gov/458831 [6] https://pubmed.ncbi.nlm.nih.gov/36684552/Check other Medicine Notes: Click here
A Visual Learning Platform



