
Cystic Hygroma Treatment – All You Need to Know
Definition
A congenital lymphatic malformation (macrocystic lymphangioma) resulting in a painless, soft, cystic mass, typically in the neck.
Pathophysiology
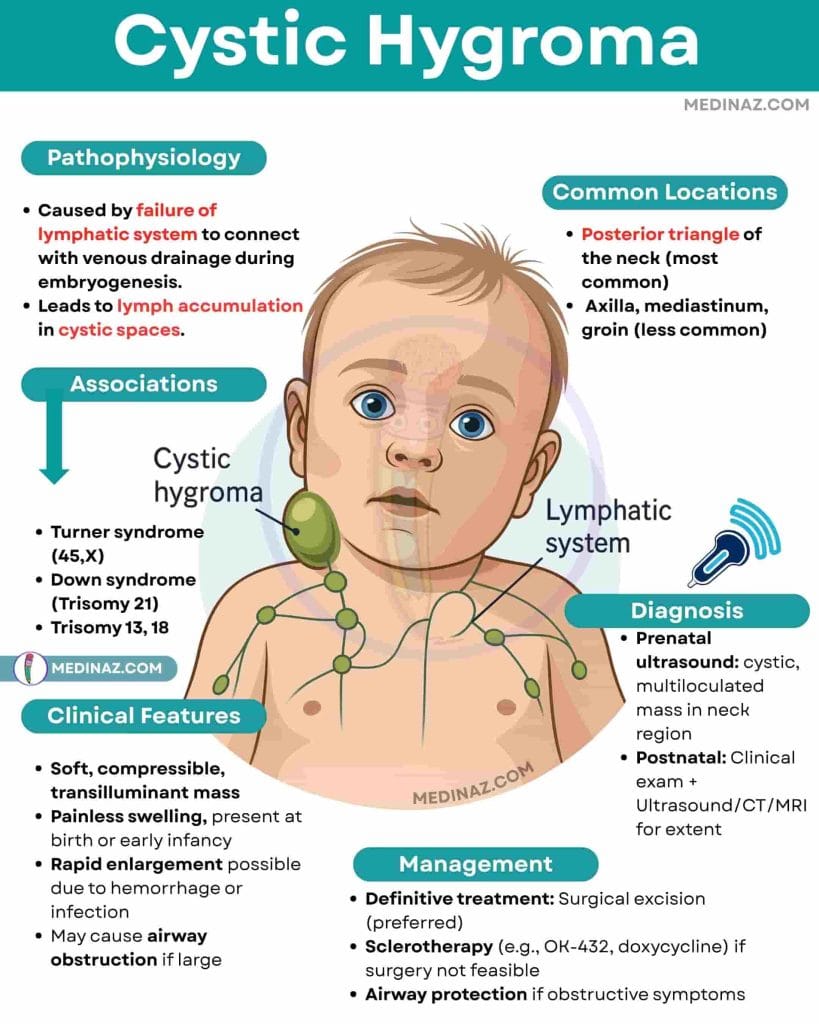
✔️ Caused by failure of lymphatic system to connect with venous drainage during embryogenesis.
✔️ Leads to lymph accumulation in cystic spaces.
Common Locations
✔️ Posterior triangle of the neck (most common)
✔️ Axilla, mediastinum, groin (less common)
Clinical Features
- Soft, compressible, transilluminant mass
- Painless swelling, present at birth or early infancy
- Rapid enlargement possible due to hemorrhage or infection
- May cause airway obstruction if large
Associations
✔️ Chromosomal anomalies:
- Turner syndrome (45,X)
- Down syndrome (Trisomy 21)
- Trisomy 13, 18
✔️ Noonan syndrome
✔️ Fetal hydrops (if large)
Diagnosis
✔️ Prenatal ultrasound: cystic, multiloculated mass in neck region
✔️ Postnatal: Clinical exam + Ultrasound/CT/MRI for extent
Management & Treatment
✔️ 1. Airway protection (First priority in large lesions)
→ If the mass causes airway obstruction (stridor, respiratory distress), ensure airway patency:
- Elective intubation may be required for stabilization.
- In extreme cases, tracheostomy may be performed to secure the airway.
- Monitor closely in the neonatal period, as rapid enlargement (e.g., due to hemorrhage or infection) can compromise breathing.
✔️ 2. Definitive treatment: Surgical Excision (Gold Standard)
→ Surgical resection is the treatment of choice for most cystic hygromas.
- Indications:
→ Symptomatic lesions (cosmetic deformity, infection, hemorrhage, or airway compression).
→ Failure of other therapies. - Timing: Delayed until infant is stable and lesion is well-defined to avoid damaging surrounding structures (nerves, blood vessels).
- Complications of surgery:
→ Injury to nearby structures (e.g., cranial nerves).
→ Risk of recurrence if complete excision is not achieved.
✔️ 3. Sclerotherapy (Alternative to surgery)
→ Used for inoperable lesions or as adjunct to surgery to shrink the mass.
- Agents:
→ OK-432 (Picibanil): most widely used.
→ Doxycycline, bleomycin, ethanol (alternative agents). - Mechanism: Induces inflammation and fibrosis within cystic spaces, leading to shrinkage.
- Advantages: Minimally invasive, fewer complications.
- Limitations: May require multiple sessions; less effective for microcystic lesions.
✔️ 4. Infection or hemorrhage management
→ Treat secondary infections with antibiotics if present.
→ Manage hemorrhage conservatively unless there is rapid enlargement or airway compromise.
Check Medinaz Book section for Highyield Visual Books
🔹 High-Yield Points
⭐ Cystic hygroma = lymphatic malformation, soft neck mass
⭐ Strong association with Turner syndrome and Down syndrome
⭐ Transilluminates on exam (differentiates from solid masses)
⭐ Can cause airway obstruction if large
⭐ Surgical excision = treatment of choice
Frequently Asked Questions:
1. What is a cystic hygroma?
✅ Answer: A cystic hygroma is a congenital lymphatic malformation (macrocystic lymphangioma) that appears as a soft, painless, and compressible mass, most commonly in the posterior triangle of the neck.
2. What causes cystic hygroma?
✅ Answer: It is caused by the failure of lymphatic channels to connect with venous drainage during embryonic development, leading to lymph accumulation in cystic spaces.
3. Where are cystic hygromas commonly located?
✅ Answer:
→ Posterior triangle of the neck (most common).
→ Other sites: axilla, mediastinum, and groin.
4. What are the clinical features of cystic hygroma?
✅ Answer:
→ Soft, painless, and compressible swelling.
→ Transilluminant on exam.
→ Can cause airway obstruction if large.
→ May rapidly enlarge due to hemorrhage or infection.
5. Which chromosomal syndromes are associated with cystic hygroma?
✅ Answer:
✔️ Turner syndrome (45,X)
✔️ Down syndrome (Trisomy 21)
✔️ Trisomy 13, Trisomy 18
✔️ Noonan syndrome
6. How is cystic hygroma diagnosed?
✅ Answer:
- Prenatal: Detected on ultrasound as a multiloculated cystic mass.
- Postnatal: Clinical examination and imaging (Ultrasound, CT, MRI) to assess extent.
- Confirmatory: Prenatal karyotyping if associated anomalies are suspected.
7. What is the treatment for cystic hygroma?
✅ Answer:
✔️ Surgical excision (Gold standard)
✔️ Sclerotherapy (OK-432, doxycycline) for inoperable or large lesions.
✔️ Airway management if obstruction occurs.
8. Can cystic hygromas resolve on their own?
✅ Answer: No, spontaneous resolution is rare. Most require surgical or sclerotherapy intervention due to risk of complications or cosmetic concerns.
9. What are the complications of cystic hygroma?
✅ Answer:
→ Airway obstruction (if large).
→ Secondary infection.
→ Hemorrhage within the cyst.
→ Recurrence after incomplete excision.
10. How is cystic hygroma prevented?
✅ Answer: There is no prevention, as it is a congenital anomaly. However, early prenatal detection allows for planning of airway management at delivery and postnatal intervention.
A Visual Learning Platform



