
Table of Contents
Tetracycline antibiotics overview:
Tetracycline antibiotics are Broad-spectrum antibiotics
The first tetracyclines were natural products derived from the fermentations of actinomycetes. (ref)
Chlortetracycline, produced by Streptomyces aureofaciens, and marketed as Aureomycin
A new synthetic subclass ‘glycylcyclines’ represented by Tigecycline has been added recently.
Tetracyclines are classified into three groups
Group I : Tetracycline, chlortetracycline, oxytetracycline
Group II : Demeclocycline, lymecycline
Group III : Doxycycline, minocycline
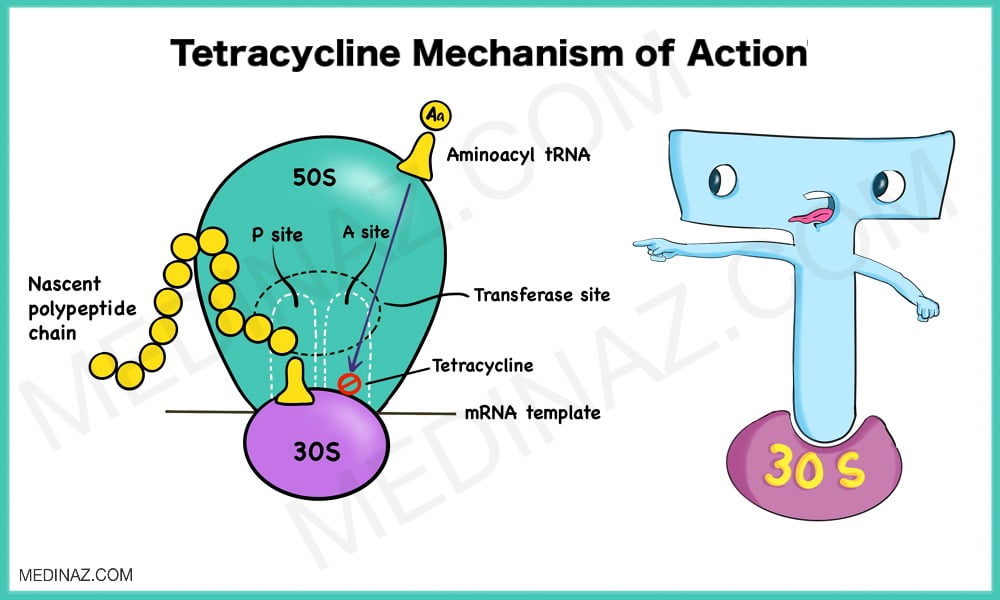
Tetracycline Mechanism of Action:
Tetracyclines are broad-spectrum bacteriostatic antibiotics that inhibit protein synthesis
Tetracyclines enter microorganisms in part by passive diffusion (more lipid-soluble members doxycycline, minocycline) and in part by an energy-dependent process of active transport
In gram-negative bacteria tetracyclines diffuse through porin channels as well
Once inside the cell, tetracyclines bind reversibly to the 30S subunit of the bacterial ribosome, blocking the binding of aminoacyl-tRNA to the acceptor site on the mRNA- ribosome complex. This prevents addition of amino acids to the growing peptide
Antimicrobial spectrum:
Tetracyclines are active against many gram-positive and gram- negative bacteria, including certain anaerobes, rickettsiae, chlamydiae, and mycoplasmas
Protozoa like Entamoeba histolytica and Plasmodium are inhibited at high concentrations
Tetracycline antibiotics resistance:
Three mechanisms of resistance:
(1) impaired influx or increased efflux by an active transport protein pump;
(2) ribosome protection due to production of proteins that interfere with tetracycline binding to the ribosome
(3) enzymatic inactivation
Pharmacokinetics of Tetracycline antibiotics:
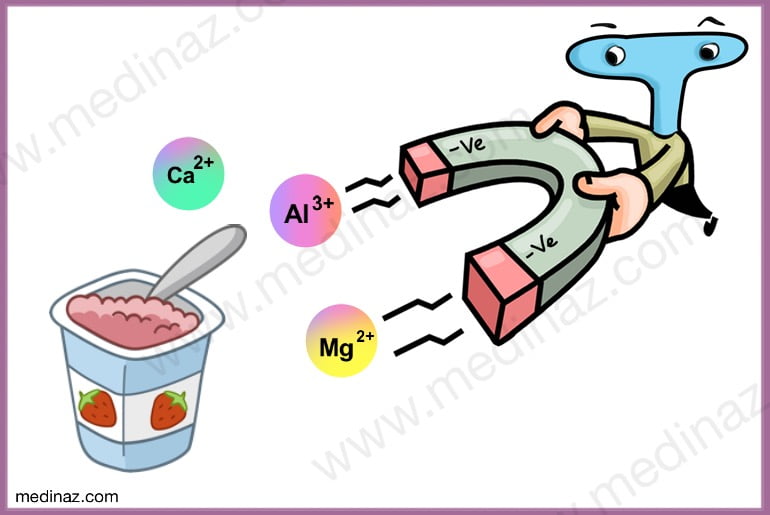
Oral absorption of tetracyclines is impaired by food and multivalent cations (calcium, iron, aluminium etc.)
Yoghurt decreases the absorption of tetracyclines because it contains cations like calcium and magnesium
Tetracyclines cross the placenta and affect the fetus, if administered to a pregnant female.
All tetracyclines undergo enterohepatic circulation
All tetracyclines are excreted primarily in the urine except doxycycline. Doxycycline is excreted in the feces and thus can be used in the presence of renal failure
Half life of doxycycline and minocycline is longer than other tetracyclines
Clinical Uses:
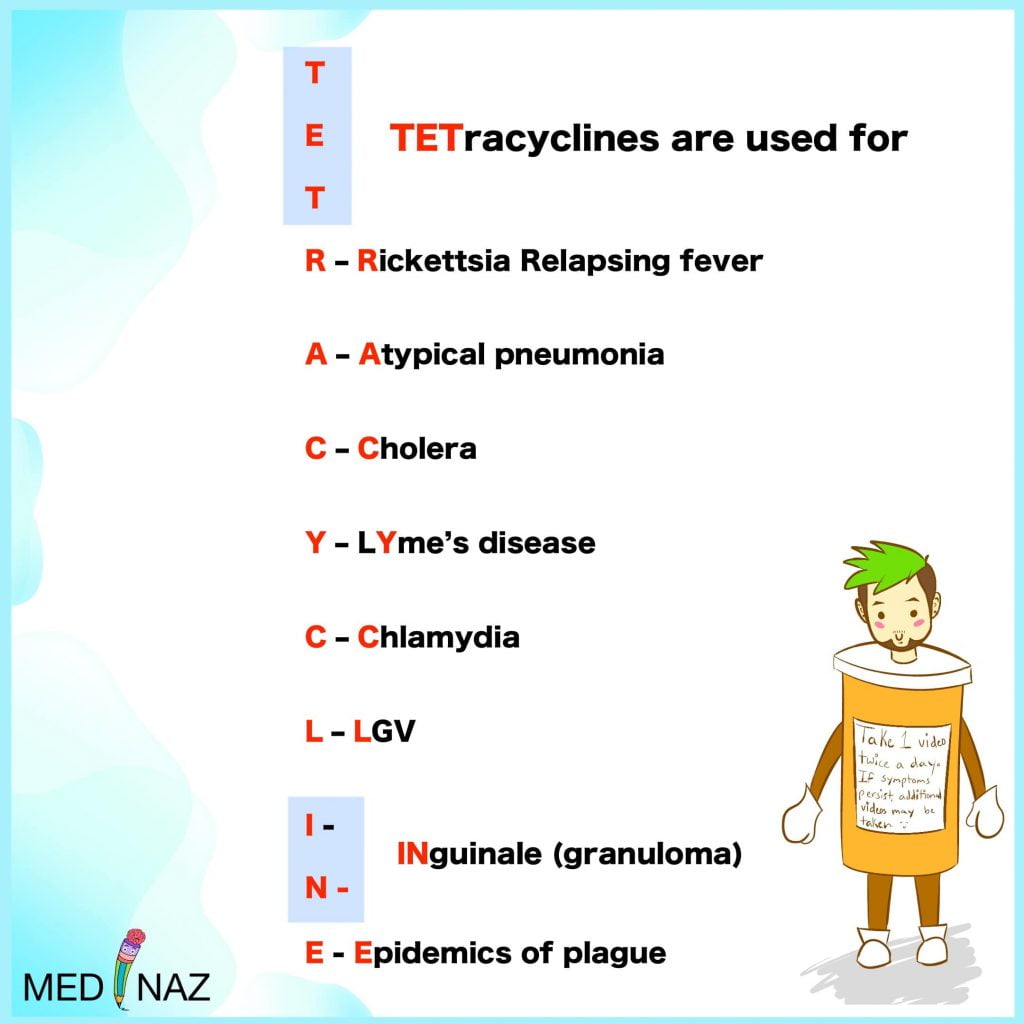
Tetracycline antibiotics are first choice drugs for
- Lymphogranuloma venereum ( LGV)
- Granuloma inguinale
- Atypical pneumonia due to chlamydia
- Cholera
- Brucellosis (with rifampicin)
- Plague prophylaxis (Drug of choice for treatment is streptomycin)
- Relapsing fever (Doxycycline)
- Lyme disease (Doxycycline)
- Rickettsial infections (Doxycycline)
- Chlamydial infections (Doxycycline)
Other uses of individual tetracyclines include
- Meningococcal carrier state (Minocycline)
- Malaria prophylaxis (Doxycycline)
- Amoebiasis (Doxycycline)
- Syndrome of inappropriate ADH secretion (Demeclocycline)
- As secondary drugs for gonorrhoea, syphilis and chlamydial infections
- For pleurodesmosis in malignant pleural effusion.
- Leprosy (minocycline)
- Peptic ulcer by H. pylori (tetracycline)
Administration of Tetracycline Antibiotics
Oral capsule is the dosage form in which tetracyclines are most commonly administered. The capsule should be taken 1⁄2 hr before or 2 hr after food.
Tetracyclines are not recommended by i.m. route because it is painful and absorption from the injection site is poor. Slow i.v. injection may be given in severe cases, but is rarely required now.
A variety of topical preparations (ointment, cream, etc.) are available, but should not be used, because there is high risk of sensitization. However, ocular application is not contraindicated.
Adverse effects of Tetracycline Antibiotics
Irritative effects
- Tetracyclines have irritant property; can cause epigastric pain, nausea, vomiting and diarrhoea on oral ingestion.
- Odynophagia and esophageal ulceration has occurred by release of the material from capsules in the esophagus during swallowing, especially with doxycycline.
- Intramuscular injection of tetracyclines is very painful; thrombophlebitis of the injected vein can occur, especially on repeated i.v. injection.
Dose related Organ toxicity
Liver damage
- Fatty infiltration of liver and jaundice occurs occasionally. Oxytetracycline and tetracycline are safer in this regard.
- Tetracyclines can precipitate acute hepatic necrosis in pregnant women
Kidney damage
- Outdated tetracycline use may lead to Fanconi’s syndrome. It is a type of renal tubular acidosis
- Tetracyclines may exacerbate pre-existing renal dysfunction although these are not directly nephrotoxic
- Doxycycine is safe in Renal failure
Phototoxicity
- A sunburn like skin reaction on exposed parts is seen in some individuals.
- More commonly seen with demeclocycline and doxycycline.
- Distortion of nails occurs occasionally
Teeth and bone defects due to Tetracycline antibiotics
- Tetracyclines have chelating property. Calcium-tetracycline chelate gets deposited in developing teeth and bone.
- Given from midpregnancy to 5 months of extra-uterine life, the deciduous teeth are affected: brown discolouration, ill-formed teeth which are more susceptible to caries.
- Tetracyclines given between 3 months and 6 years of age affect the crown of permanent anterior dentition.
- In UV rays it shows bright yellow fluorescence
- Doxycycline is less likely to cause this adverse effect.
- Minocycline hydrochloride, a synthetic derivative of tetracycline may affect fully developed teeth (ref)
- Repeated courses are more damaging.
- Given during late pregnancy or childhood, tetracyclines can cause temporary suppression of bone growth.
Antianabolic effect
- Tetracyclines reduce protein synthesis and have an overall catabolic effect. They induce negative nitrogen balance and can increase blood urea.
Intracranial pressure
- Increased intracranial pressure is noted in some infants.
Diabetes insipidus
- Demeclocycline antagonizes ADH action and reduces urine concentrating ability of the kidney.
- It has been tried in patients with inappropriate ADH secretion.
Vestibular toxicity
- Minocycline can cause ataxia, vertigo and nystagmus, which subside when the drug is discontinued.
Hypersensitivity
- This is infrequent with tetracyclines. Skin rashes, urticaria, glossitis, pruritus, exfoliative dermatitis have been reported.
- Angioedema and anaphylaxis are extremely rare.
Superinfection
- Tetracyclines may cause superinfection diarrhea and pseudomembranous colitis. Gastrointestinal side effects are most common adverse effects.
- Doxycycline and minocycline are less liable to cause diarrhoea, because only small amounts reach the lower bowel in the active form.
Precautions
- Tetracycline antibiotics should not be used during pregnancy, lactation and in children.
- They should be avoided in patients on diuretics: blood urea may rise in such patients.
- They should be used cautiously in renal or hepatic insufficiency.
- Preparations should never be used beyond their expiry date.
- Do not mix injectable tetracyclines with penicillin—inactivation occurs.
- Do not inject tetracyclines intrathecally.
Reference:
Basic and Clinical Pharmacology; Bertram G. Katzung; 14th ed
The Pharmacological Basis of Therapeutics; Goodman & Gilman’s; 13th ed
Essentials of Medical Pharmacology; KD Tripathi; 7th ed
Review of Pharmacology; Garg & Gupta; 14th ed
A Visual Learning Platform



