
Oral manifestations of vitamin deficiency illustrated high yield Oral medicine notes
Table of Contents
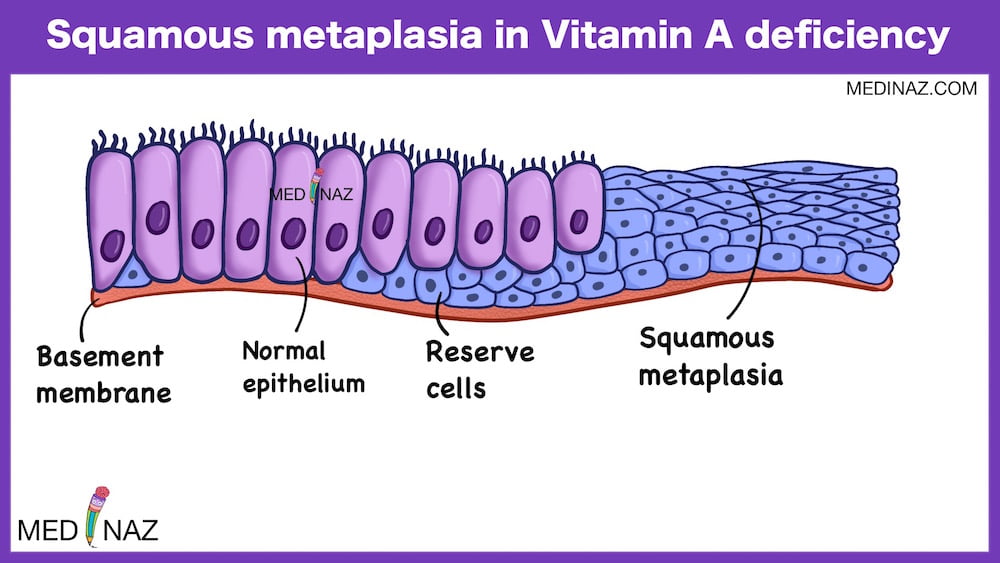
Oral manifestations of Vitamin A deficiency
- Keratinizing metaplasia of epithelium resulting in increased keratin formation
- Occlusion of salivary gland ducts with keratin
- Enamel hypoplasia, atypical dentin formation and epithelial invasion of pulpal tissue are characteristic features
- It affects Enamel more seriously than dentin
- Delayed eruption of teeth
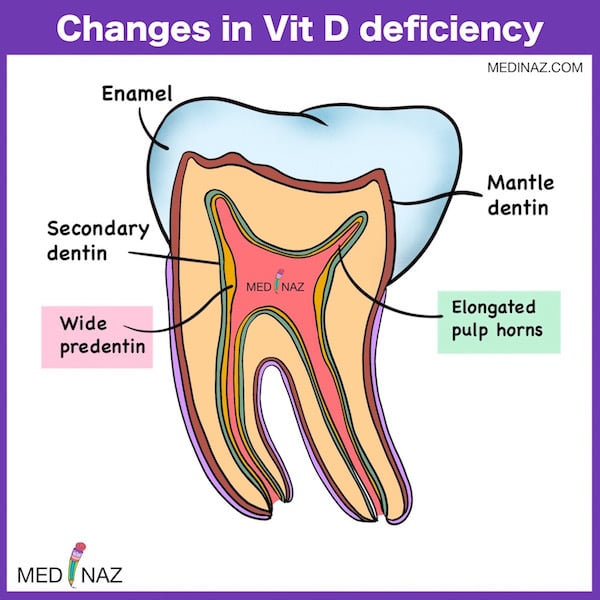
Oral manifestations of Vitamin D deficiency
- Delayed eruption of primary and permanent teeth
- Malalignment of the teeth in the Jaws
- Developmental anomalies of dentin and enamel of the teeth shows wide pre dentine zone with much interglobular dentin
- The pulp horns are elongated and extend high, reaching the DE junction
- The enamel does not appear to be weekend but the rough surface may facilitate adherence of dental plaque and food Residue.
Vitamin K deficiency
- Prothrombin level (below 35%) results in gingival bleeding after tooth brushing
- Spontaneous gingival bleeding occurs when the prothrombin levels fall <20%
- Spontaneous bleeding during minor dental, surgical procedure
Vitamin C deficiency
- The pathognomonic sign is swollen and spongy gums, particularly the intendental papilla is involved producing the appearance of scurvy buds
- In severe cases, hemorrhage to periodontal membrane, weakened collagen formation followed by resorption of alveolar bone and loosening of teeth occurs.
- Scurvy occurs in as quickly as 20 days
- Gingival hemorrhage and petechiae are also evident
- Scrobutic changes in the teeth because of changes in ameloblasts and odontoblasts also seen
- Trismus due to hemorrhage in TMJ

Vitamin B1 (Thiamin) deficiency
- Flabby, red and edematous tongue
- The fungiform papillae enlarge and become hyperemic
- Gingival tissue sometimes present an “old rose” color.
Vitamin B2 (Riboflavin) deficiency
- Glossitis- The filiform papillae become atrophic while the fungiform papillae become engorged and mushroom shaped, resulting in magenta coloured tongue
- Angular cheilosis and ocular lesion
- Non-specific bilateral angular cheilosis may be seen in association with faulty dentures or in patient with reduced vertical dimension due to attrition
- Lips may become extremely red and smooth
Vitamin- B3 (niacin) deficiency
- Bald tongue with Sandwith on Raw beefy tongue due to loss of filliform and fungiform papillae
- Oral mucosa become fiery red and painful
- Painful stomatitis causes diminished food intake
- Pellagrous glossitis begins with swelling of the papillae at the tip of the tongue and lateral borders
- Salivation is profuse
Vitamin -B6 (Pyridoxine) deficiency
- Pyridoxine deficiency induced glossitis is associated with pain, edema and papillary changes
- Initially the tongue has a scalded sensation, followed by reddening and hypertrophy of the filliform papillae at the tip, margins and dorsum.
Folic acid deficiency deficiency
- Glossitis – Tongue becomes fiery red and papillae are absent.
- Initially filliform papilla are involved and in advanced cases fungiform papillae are involved
- Marked chronic periodontitis and loosening of tooth
- Superimposed candidiasis is due to impaired immune response of mucosa.
Ora manifestations of Vitamin B 12 deficiency
- Beefy red tongue with glossopyrosis, glossitis and glossodynia.
- Hunter’s glossitis or Moeller’s glossitis which is similar to Bald tongue of Sandwith seen in Pellagra.
- An oral examination may reveal stomatitis on a pale or yellowish mucosa, Xerostomia, cheilosis, Hemorrhage gingiva and bone loss.

Biotin deficiency
- Pallor of the tongue and patchy atrophy of the lingual papillae
- Although pattern resembles geographic tongue it is continued to lateral margins is generalised to the entire dorsum.
Reference:
Oral and maxillofacial pathology; Neville; 4th ed
Shafer’s Textbook of Oral Pathology
Burket’s Oral Medicine; 12th ed
A Visual Learning Platform



