
Ameloblastoma Radiology: Illustrated Dental Notes for NBDE, NEET MDS and Dental Board Exams
Ameloblastoma Radiology: Commonly affected areas:
Mandible – 80% develop in the molar-ramus region of the mandible, but may extend to the symphyseal area. (ref)
Maxilla – it is more common in the third molar region and may extend into the maxillary sinus and nasal floor.
In either jaw the tumor usually originates in an occlusal position to a developing tooth.
Periphery of the lesion:
It usually has a well-defined and frequently delineated by a corticated border, which is curved an in small lesions the border and shape may be indistinguable from a cyst.
The periphery of the lesion in the maxilla is more ill-defined.
Ameloblastoma Internal structures:
The internal structure varies from totally radiolucent to mixed with presence of bony septa
The septa can be straight but are more commonly “coarse” or “curved”
The septa is originated from normal bone that has been trapped within the tumor
Radiological variants of Ameloblastoma:
H.M. Worth described 4types of appearances:
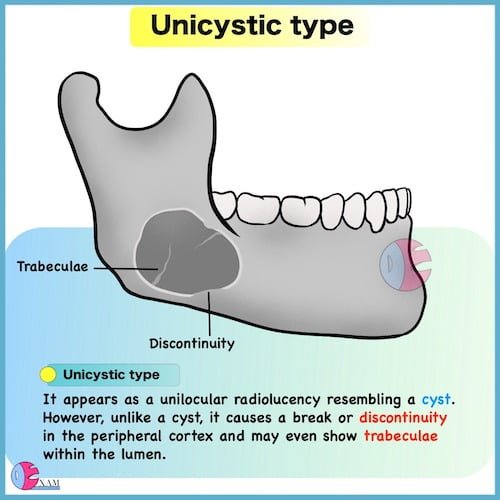
Unicystic type ameloblastoma:
It appears as a unilocular radiolucency resembling a cyst. However, unlike a cyst, it causes a break or discontinuity in the peripheral cortex and may even show trabeculae within the lumen.
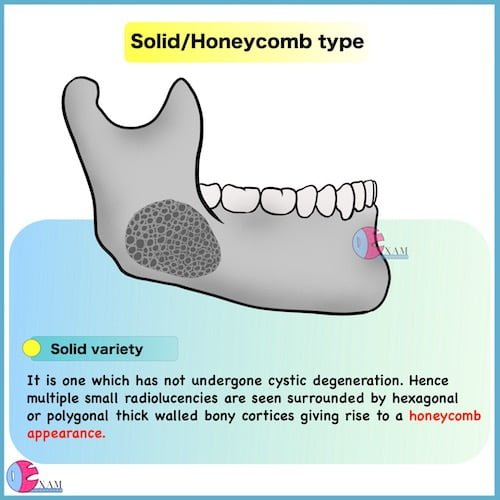
Solid/honeycomb type ameloblastoma:
It is one which has not undergone cystic degeneration. Hence multiple small radiolucencies are seen surrounded by hexagonal or polygonal thick walled bony cortices giving rise to a honeycomb or soap bubble appearance. The jaw may be expanded laterally and inferiorly. An unerupted tooth may be present
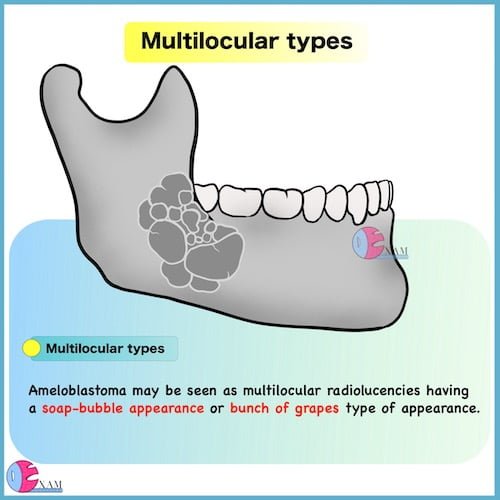
Multilocular type ameloblastoma:
Ameloblastoma may be seen as multilocular radiolucencies having a soap-bubble appearance or bunch of grapes type of appearance.
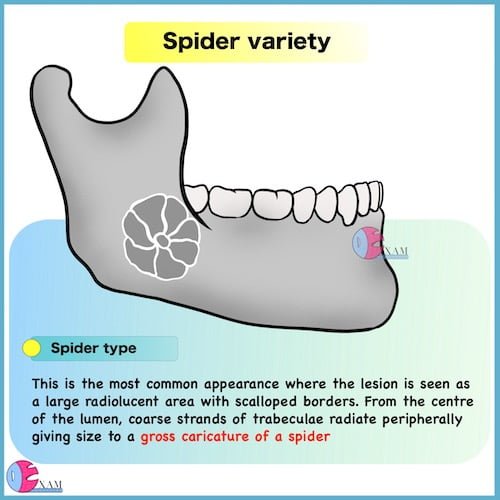
Ameloblastoma Spider Variety:
This is the most common appearance where the lesion is seen as a large radiolucent area with scalloped borders. From the centre of the lumen, coarse strands of trabeculae radiate peripherally giving size to a gross caricature of a spider
- A subclinical lesion, usually presents in radiographs as many small rounded cavities in bone having sharply defined and sometimes corticated borders. In some cases there are two rounded and well-defined small cavities having good bony cortex; in the center of which there is a small white dot.
Effects on surrounding structures:
Extensive root resorption and tooth displacement is common.
The displacement is of the tooth is apically.
An occlusal radiograph may demonstrate cyst like expansion and thinning of an adjacent cortical plate, leaving a thin egg-shell of bone.
Actual perforation of bone into the surrounding tissues or anatomical spaces is a late feature of ameloblastoma.
Unicystic types may cause extreme expansion of the mandibular ramus and often the anterior border of the ramus is not visible in the panaromic radiograph.
Recurrent ameloblastoma (inadequate resection) has a characteristic appearance of multiple small cyst like structures with very coarse sclerotic cortical margins, sometimes separated by normal.
Ameloblastoma Radiology: Additional Imaging
CT not only helps to confirm the diagnosis but also accurately demonstrates the anatomical extent of the tumor. It helps to detect perforation of the outer cortex and invasion into the surrounding soft tissues. It is also important for the post surgical follow-up assessement.
CT findings in ameloblastoma consist of low attenuation cystic areas intermixed with isodense areas reflecting the solid component of the lesions. The size of the low attenuation cyst may vary from small to large. The expanding lesion may cause a thin bony rim at the periphery.
MRI provides superior images of the nature and extend of invasion in the soft tissues.
Differential diagnosis of Ameloblastoma:
Small and unilocular ameloblastoma: These are located around the crown of an unerupted tooth often cannot be differentiated from a dentigerous cyst.
Residual cyst: There is history of extraction of the tooth.
Lateral periodontal cyst: It is found in incisor, canine and premolar area in the maxilla, ameloblastoma occurs more in the mandibular molar area.
Giant cell granuloma: It is found more often in areas anterior to the molars, younger age group and have more granular and ill-defined septae.
Traumatic bone cyst: This occurs in the mid twenties, whereas ameloblastoma is more common in the 3rd and 4th decades.
Primordial cyst: Same as traumatic bone cyst:
Odontogenic keratocyst: Contains curved septae but tends to grow along the bone without marked expansion. In case of ameloblastoma there will be significant bony expansion.
Odontogenic myxoma: There is history of missing tooth and has a presence of septa that divide the image into much finer coarse than those in ameloblastoma. Myxoma has one or two thin, sharp, straight septa which are characteristic of it. Myxomas are not expansile and tend to grow along the bone.
Ossifying fibroma: The septa are usually wide, granular and ill-defined. Small irregular trabeculae are seen.
“Visual Book of Odontogenic Tumor” is now available on “Medinaz” App. The App is available on Appstore & Playstore. Visit our website www.medinaz.com for other available books.
Book overview:
– All the necessary High-Yield Points
– 550+ Frequently tested facts
– 300+ hand drawn Images
– Mnemonics to remember
– Helpful for: NBDE, NEET MDS, and Board exams
– FREE UPDATES up to 1 year from the date of publish
– (Time span to be counted from the day it was published)
– Neatly organized materials
– Lifetime access
– Format Image based PDF
Ameloblastoma Radiology Reference:
Oral radiology Principles and Interpretation; White & Pharoah
Essentials of Oral and Maxillofacial Radiology; F. Karjodkar
Concise Oral Radiology; HR Umarji
A Visual Learning Platform



