
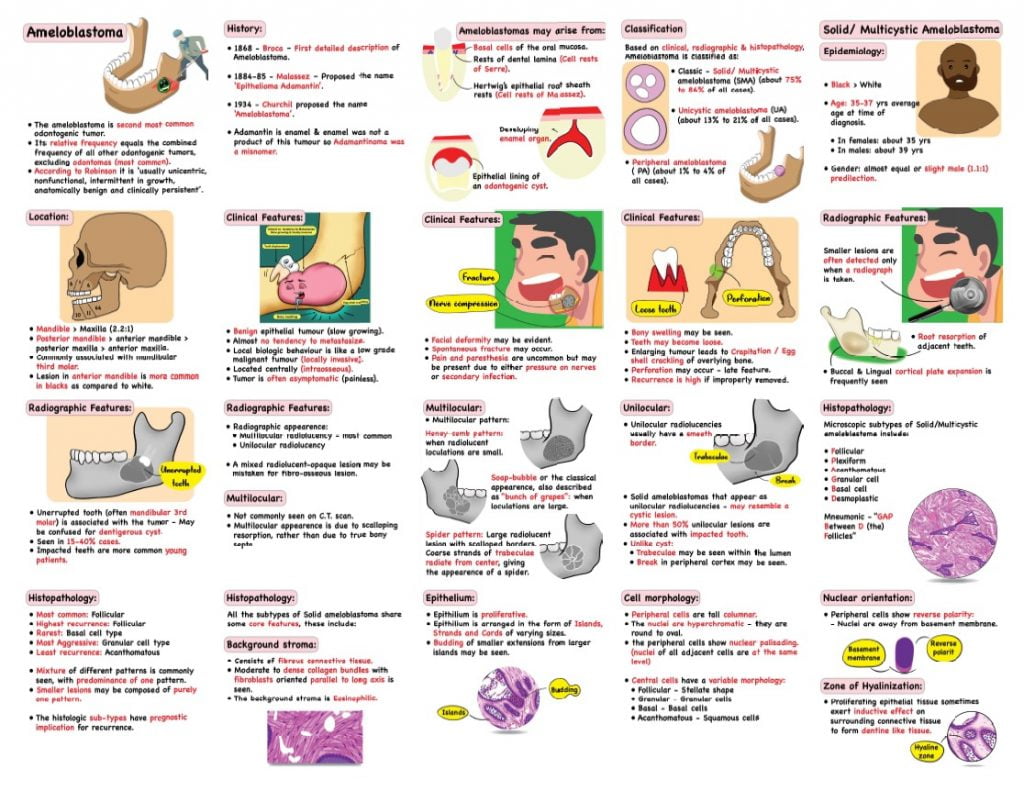
Classification of Ameloblastoma:
Based on clinical, radiographic & histopathology & behavioural & prognostic aspects, Ameloblastoma is classified as:
- Classic- Solid/ Multicystic ameloblastoma (SMA)
- Unicystic ameloblastoma (UA)
- Peripheral ameloblastoma (PA)
- Desmoplastic ameloblastoma (DA), including hybrid lesion.
Solid/ Multicystic Ameloblastoma (SMA)
Clinical Features:
- Benign epithelial tumour, with almost no tendency to metastasize. Though it is locally invasive.
- High recurrence if improperly removed
- Located centrally (intraosseous).
- Few or no clinical signs in early stages.
- Later signs:
- Facial deformity, loose teeth
- Spontaneous fracture may be seen.
- Bony swelling may be seen
- Pain: Due to either pressure of growing tumour on nerves or secondary infection.
- Enlarging tumour makes the surrounding bone elicit Crepitation/ Egg shell crackling
- Perforation of bone may occur.
Radiographic features:
- Multilocular lesion- typical appearance
- Unilocular may also be seen.
- Unilocular:
- Well defined single radiolucency.
- If associated with unerupted tooth, may resemble Dentigerous cyst or OKC.
Epidemiology:
- Black> White
- Age– 35-37 yrs average age at time of diagnosis.
- According to Gardener, mean age at time of diagnosis:
- SMA– about 39 yrs
- Unicystic– about 22 yrs
- Peripheral– about 51 yrs
- Gender– almost equal or slight male (1.1:1) predilection.
- Location: Mandible> Maxilla (2.2:1)
- Posterior mandible> anterior mandible> posterior maxilla> anterior maxilla
Pathology:
Pathogenesis:
- Mostly arise from odontogenic epithelial remnants, specifically remnants of dental lamina.
- If these remnants lie outside bone in soft tissues, they form Peripheral Ameloblastoma.
- May arise as neoplastic change in lining or wall of cysts like Dentigerous or OKC called Mural ameloblastoma. (usually seen in posterior region).
- May originate from Epithelial rests of Malassez.
Microscopy:
WHO 1992 definition: A polymorphic neoplasm consisting of proliferating odontogenic epithelium which usually has a follicular or plexiform pattern lying in a fibrous stroma.
The various histologic patterns of SMA include:
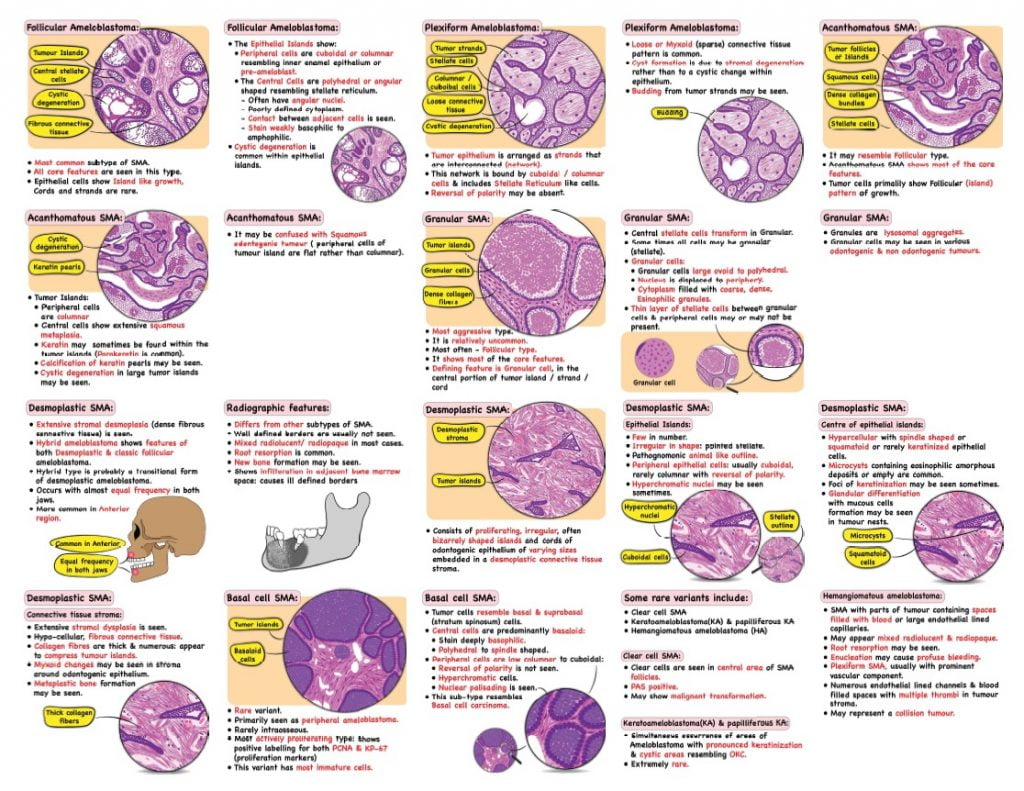
Follicular pattern
- Epithelial Islands: Contain central mass of polyhedral cells, or loosely connected angular cells resembling stellate reticulum.
- Peripheral cells in the epithelial islands are cuboidal or columnar resembling inner enamel epithelium or pre-ameloblast.
- Cystic degeneration is common within epithelial islands
Plexiform pattern
- Tumour epithelium arranged as a network
- This network bound by cuboidal to columnar cells & includes Stellate Reticulum like cells.
- Cyst formation is due to stromal degeneration may be seen.
- Hyaline bodies like odontogenic cyst epithelium/wall may be seen
Acanthomatous SMA:
- Extensive squamous metaplasia
- Keratin may be formed sometimes (within tumour island)
- Generally, shows follicular pattern
- Third most common histologic type.
Granular cell SMA:
- Most often it shows Follicular pattern.
- Granular transformation of central stellate cells.
- Granular cells may be Cuboidal, Columnar or Round.
- Cytoplasm filled with Acidophilic granules.
- Granularity may be due to increased apoptosis & phagocytosis of cells by neighbouring neoplastic cells.
Desmoplastic SMA:
- Usually follicular pattern of SMA
- Connective tissue shows marked hyalinization (desmoplasia).
Basal cell SMA:
- Resemble basal & suprabasal spinosum cells.
- Rare variant
- SMA shows predominant basaloid pattern.
- Most actively proliferating type. It shows positive labelling for bothPCNA & KP-67.
- This variant has most immature cells.
Clear cell SMA:
- Clear cells in stellate cell area of SMA follicles
- PAS positive
- May show malignant transformation.
Keratoameloblastoma(KA) & papilliferous KA:
- Simultaneous occurrence of areas of Ameloblastoma with pronounced keratinization & cystic areas of resembling OKC.
- Extremely rare.
Connective tissue of all histologic variants of SMA:
- Contains fibroblasts, collagen fibres & myofibroblasts.
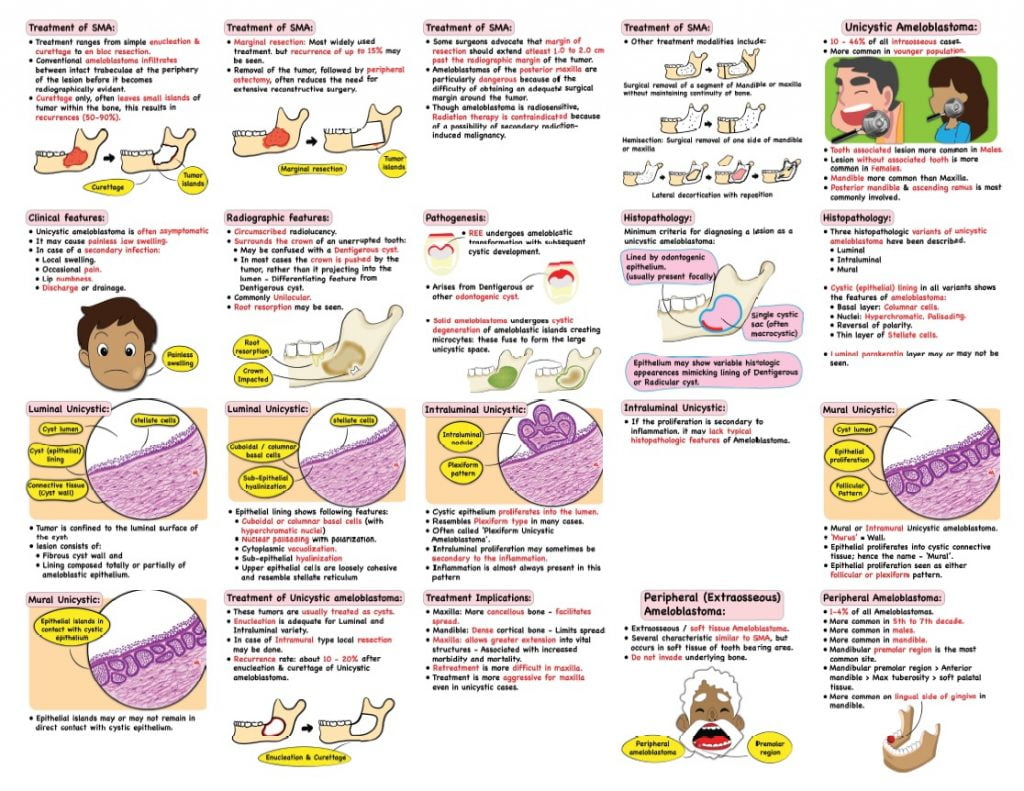
Treatment:
- Treatment ranges from simple enucleation and curettage to en bloc resection.
- Curettage only, often leave small islands of tumor within the bone, this results in recurrences (50-90%).
- Marginal resection: Most widely used treatment, but recurrence of up to 15% may be seen.
- Removal of the tumor, followed by peripheral ostectomy, often reduces the need for extensive reconstructive surgery.
- Ameloblastomas of the posterior maxilla are particularly dangerous because of the difficulty of obtaining an adequate surgical margin around the tumor.
- Though ameloblastoma is radiosensitive, Radiation therapy is contraindicated because of a possibility of secondary radiation-induced malignancy.
Unicystic Ameloblastoma
- Well defined, often large monocystic cavity with a lining.
- Locally but rarely entirely lined by odontogenic epithelium.
- On the Luminal surface of cyst, one or several polypoid or papillomatous, pedunculated exophytic masses may be seen: These are called Intracystic, Luminal or Intraluminal ameloblastoma.
- Epithelial nodules may grow within the connective tissue: Called Mural or Intramural.
- May be associated with an unerupted tooth.
Clinical & Radiographic findings:
- If there is secondary infection:
- Local swelling
- Occasional pain
- Lip numbness
- Discharge or drainage
- May be unilocular or multilocular; Unilocular more common
- Root resorption is common.
- If crown of unerupted tooth is involved, it is displaced by cystic tumour rather than project into cystic lumen – Differentiation from Dentigerous cyst.
Epidemiology:
- Tooth associated lesion occurs in younger patients compared to those not associated with tooth.
- Males: Tooth associated lesion more common; Females: Lesion without tooth are common.
- Mandible > Maxilla; Posterior mandible & ascending ramus is most commonly involved.
Pathology:
Pathogenesis:
- May arise from pre-existing odontogenic cyst (commonly Dentigerous cyst) or it may arise de novo.
- According to Leider et al.: They may arise from:
- From REE.
- From Dentigerous or another odontogenic cyst.
- From Solid ameloblastoma undergoing cystic degeneration.
Microscopy:
- Minimum criteria for diagnosing a lesion a unicystic ameloblastoma:
- Single cystic sac.
- Lined by odontogenic epithelium (usually present locally).
- Epithelium may be variable, mimicking lining of Dentigerous or Radicular cyst.
Sub-groups of unicystic ameloblastoma:
Luminal type:
- Epithelial lining may show transformation to cuboidal or columnar basal cells.
- Nuclear palisading with polarization.
- Cytoplasmic vacuolization.
- Intercellular spacing.
- Sub-epithelial hyalinization.
Intramural tissue:
- Infiltration from cyst lining or as free islands of follicles (SMA) often with central cystic degeneration.
- About 2/3 of both tooth-associated & non-tooth-associated show intramural invasion.
- Though slightly more common in non-tooth type.
- Intra luminal proliferation more common in tooth associated type.
- Tumours with intramural invasion have higher recurrence.
Treatment:
- May be treated conservatively by enucleation or it may need aggressive treatment as classic SMA, depending on the histopathologic presentation.
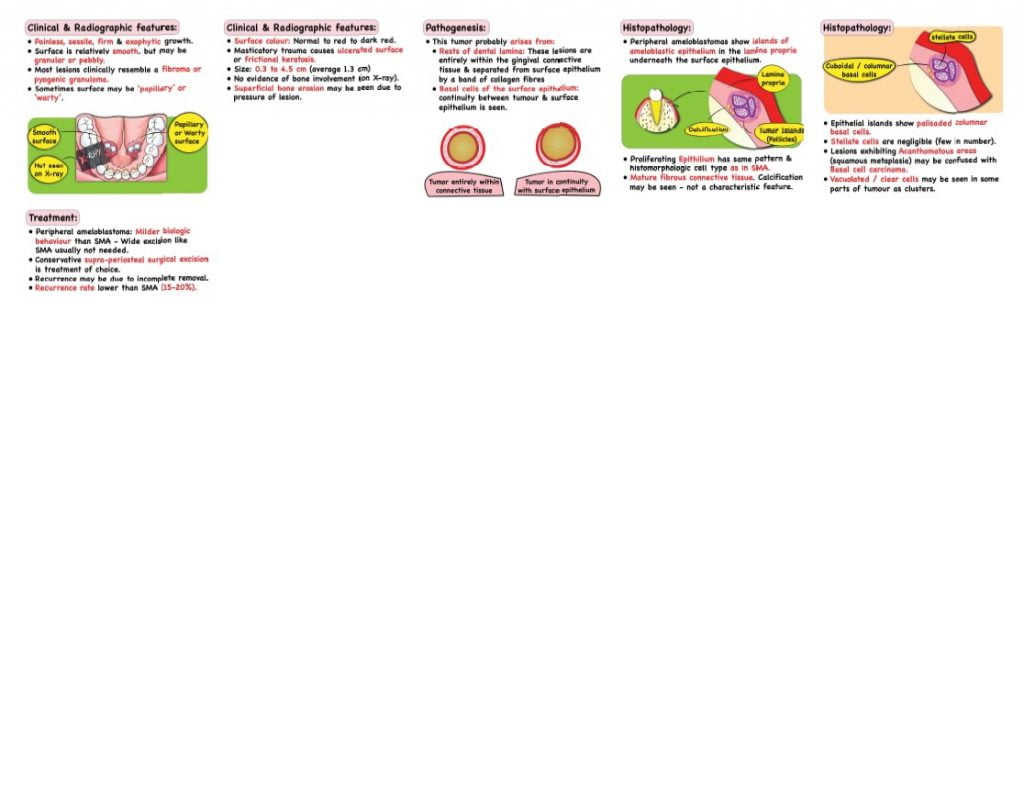
Peripheral Ameloblastoma:
- Peripheral ameloblastoma is a benign neoplasm or hamartomatous lesion confined to soft tissue overlying tooth bearing area of jaws.
- Several characteristic similar to SMA.
- Do not invade underlying bone.
Clinical & Radiographic features:
- Painless, sessile, firm & exophytic growth.
- Surface is relatively smooth, but may be granular or pebbly. Sometimes Papillary or Warty.
- Surface colour: Normal to red to dark red.
- Size– 0.3 to 4.5 cm (1.3 cm)
- Superficial bone erosion may be seen, due to pressure of lesion.
Epidemiology:
- 2-10% of all Ameloblastomas.
- Age– 9-92 yrs. (Average age: 52 yrs.). More common in 5th to 7th decade.
- Gender: more common in males.
- Location: more common in mandible. Mandibular premolar region most common site.
Pathology:
Pathogenesis:
- Probably arises from dental lamina remnants. (cell rests of Serre).
- May also arise from surface epithelium. Continuity between tumour & surface epithelium has been seen.
Microscopy:
Epithelium:
- Epithelial islands show palisaded columnar basal cells.
- Stellate reticulum like cells are few in number (negligible).
- Lesions exhibiting Acanthomatous areas are difficult to distinguise from Basal cell carcinoma.
- Ghost cells in Acanthomatous area may be seen. May be confused with Calcifying ghost cell odontogenic cyst.
- Vacuolated or clear cells may be seen in some parts of tumour as clusters.
Stroma:
- Mature fibrous connective tissue (calcification may be seen sometimes).
Treatment:
- It exhibits a milder biologic behaviour than the SMA. So, wide excision is usually not needed.
- Conservative supra-periosteal surgical excision with adequate disease-free margins.
- Recurrence rate lower than SMA.
Desmoplastic Ameloblastoma
- Extensive stromal collagenisation or desmoplasia.
- Hybrid ameloblastoma: Shows features of both Desmoplastic variant & classic follicular ameloblastoma. It is probably a transitional form of desmoplastic ameloblastoma.
Clinical features:
- Benign, locally infiltrative, epithelial neoplasm.
- A variant or sub-type of SMA.
- Painless swelling: chief complaint in most cases.
Radiographic features:
- Well defined borders are usually not seen.
- Mixed radiolucent/ radiopaque in most cases.
- Root resorption is common.
- New bone formation may be seen.
- Shows infiltration in adjacent bone marrow space. It causes ill-defined borders of lesion.
Epidemiology:
- 4-13% of all SMA
- Age – 17-72yrs (43yrs)
- Slight or no male predominance.
- Occurs with almost equal frequency in both jaws. More common in Anterior region.
Pathogenesis:
Microscopy:
- Consists of proliferating, irregular, often bizarrely shaped islands and cords of odontogenic epithelium of varying sizes embedded in a desmoplastic connective tissue stroma.
Epithelial islands:
- Irregular in shape and have a pointed stellate appearance.
- Pathognomonic animal like outline.
- Peripheral epithelial cells are usually cuboidal, rarely columnar with reversal of polarity.
- Hyperchromatic nuclei may be seen sometimes.
Centre of epithelial islands:
- Hypercellular with spindle shaped or squamatoid or rarely keratinized epithelial cells.
- Microcysts containing eosinophilic amorphous deposits or empty are common within tumour islands.
- Foci of keratinization may be seen sometimes.
- Glandular differentiation with mucous cells formation may be seen in tumour nests.
Connective tissue stroma:
- Extensive stromal dysplasia.
- Moderately cellular, fibrous connective tissue.
- Collagen fibres are thick & numerous. They appear to compress tumour islands.
- Myxoid changes may be seen in stroma around odontogenic epithelium.
- Metaplastic bone formation may be seen.
- Capsule – peripheral fibrous condensation not always seen.
Treatment:
Same as SMA
“High Yield Visual Book of Dental Cyst” is now available on “Medinaz” App. The App is available on Appstore & Playstore. Visit our website www.medinaz.com for other available books.
Book overview:
– All the necessary High-Yield Points
– 550+ Frequently tested facts
– 300+ hand drawn Images
– Mnemonics to remember
– Helpful for: NBDE, NEET MDS, and Board exams
– FREE UPDATES up to 1 year from the date of publish
– (Time span to be counted from the day it was published)
– Neatly organized materials
– Lifetime access
– Format Image based PDF
Check other Dental Notes: Click here
A Visual Learning Platform



