
What is Ramsay Hunt Syndrome?
Ramsay Hunt syndrome is a rare neurological disorder that causes facial paralysis and a rash around the ear. It is caused by the varicella-zoster virus (VZV), the same virus that causes chickenpox and shingles.
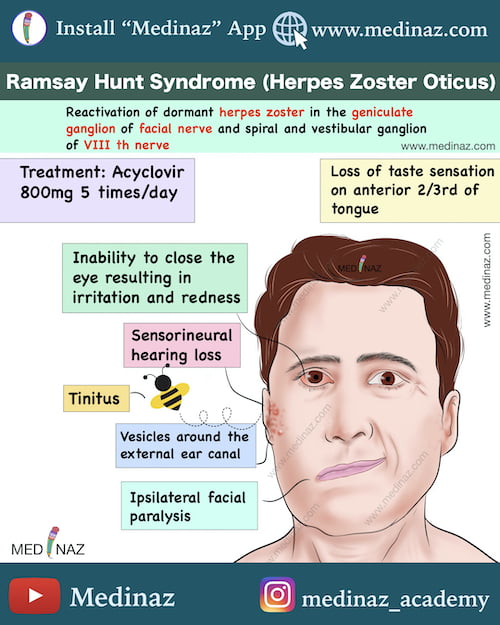
Signs & symptoms of Ramsay Hunt Syndrome:
The most common signs and symptoms of Ramsay Hunt syndrome are:
- Facial paralysis on one side of the face (ipsilateral)
- Loss of taste sensation in the anterior 2/3rd of the tongue
- A rash with fluid-filled blisters around the ear, on the face, or in the mouth
- Pain in the ear, face, or jaw
- Hearing loss
- Tinnitus (ringing in the ears)
- Vertigo (dizziness)
- Nausea and vomiting
Causative agent:
Ramsay Hunt syndrome is caused by the varicella-zoster virus (VZV). VZV is a common virus that causes chickenpox in children. After chickenpox clears up, the virus stays dormant in the body’s nerve cells (geniculate ganglion).
In some people, the virus can reactivate years later and cause shingles. When shingles affects the facial nerve, it can lead to Ramsay Hunt syndrome.
Pathophysiology of Ramsay Hunt Syndrome:
- The pathophysiology of RHS is believed to be a consequence of herpes zoster inflammation of the geniculate ganglion, with either direct extension to involve areas of the nerve trunk or secondary pressure effects from the inflamed ganglion on the nerve trunk (ref)
- Varicella-zoster virus (VZV) causes chickenpox initially and can remain dormant in cranial nerves and dorsal root ganglia.
- Reactivation of VZV within the geniculate ganglion leads to RHS, primarily affecting the facial nerve.
- Typical initial symptoms include ipsilateral ear pain, followed by facial paralysis and vesicles within 2 to 3 days.
- Rashes can appear on the auricle, oral cavity, scalp, and cheek.
- Proximity to the vestibulocochlear nerve can result in hearing loss, tinnitus, and vertigo.
- Vagal nerve involvement may occur, but it is often asymptomatic unless assessed with laryngoscopy.
- Other cranial nerves like trigeminal, glossopharyngeal, and hypoglossal may also be affected, especially in immunocompromised patients. (ref)
Management:
Ramsay Hunt Syndrome is Self limiting in nature. Treatment typically includes:
Antiviral Medications:
Antiviral medications, such as acyclovir(500 mg five times a day), valacyclovir (1000 mg three times a day) or famciclovir (500 mg three times a day)
Antiviral treatment is usually administered for 7 to 10 days; in some cases 21 days
Steroids:
High dose of Steroids, such as prednisone 1 mg/kg/day (up to 60 mg maximum dose) or equivalent, followed by a taper to prevent acute adrenal insufficiency
Intratympanic injection is another modality for corticosteroid treatment, delivering steroids topically to the affected area.
Pain medication:
Analgesia is often necessary for zoster, and a multimodal approach can be used, including acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), and long-acting opioids.
Tricyclic antidepressants and gabapentin are effective for treating neuropathic pain and postherpetic neuralgia.
Physical therapy
Meclizine and benzodiazepines can help manage acute vertigo.
Artificial tears during the day and ocular lubricant ointment at night are helpful in preventing exposure keratopathy.
Complications:
The most serious complication of RHS is permanent facial paralysis. Other complications can include hearing loss, tinnitus, vertigo, and difficulty eating.
Prognosis:
The prognosis for RHS is generally good. Most people with the condition make a full recovery within a few weeks or months. However, some people may experience permanent facial paralysis or hearing loss.
Check the other Medinaz Visual Notes: Click here
A Visual Learning Platform



