
This Acute Liver Failure Pathology: HY Note covers all the necessary High-yield points for your exam preparation
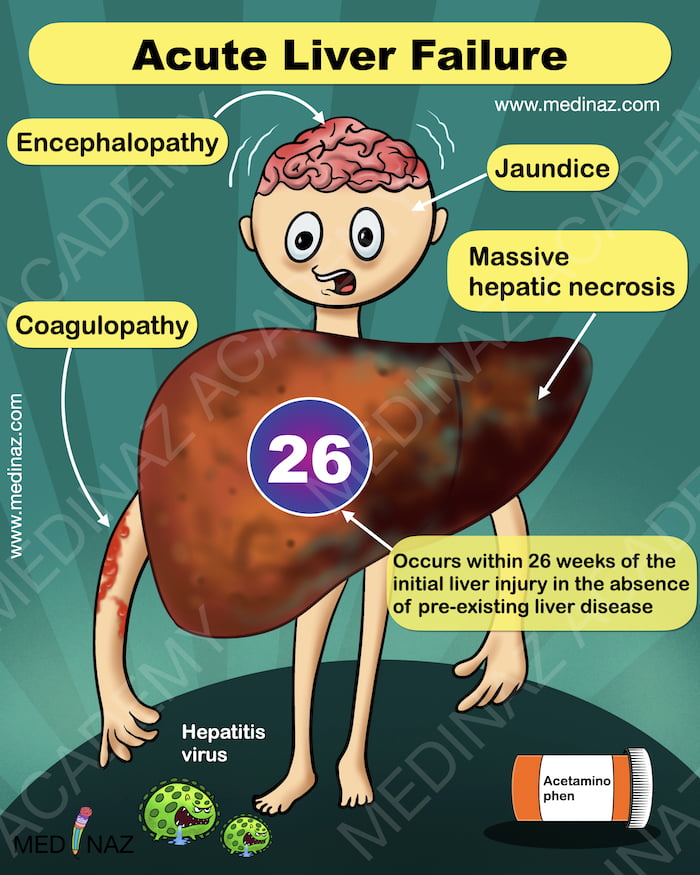
- Acute liver failure is characterized by acute liver illness accompanied by encephalopathy and coagulopathy within 26 weeks of the initial liver injury, without preexisting liver disease.
- The syndrome typically manifests within 8 weeks of injury, with many patients progressing to coma within a week.
- The interval between symptom onset and liver failure can provide clues to the underlying cause within the 26-week window.
- Rapid onset acute liver failure is commonly induced by drugs or toxins, resulting in massive hepatic necrosis.
- “Fulminant liver failure” is an older term for this form of liver failure, still used interchangeably.
- Acetaminophen ingestion is the leading cause of adult cases in the United States, accounting for almost 50%.
- Autoimmune hepatitis, other drugs/toxins, and acute hepatitis A and B infections are other common causes.
- In Asia, acute hepatitis B and E are the predominant causes.
- Acetaminophen toxicity leads to liver failure within 1 week of symptom onset, while hepatitis viruses take longer to develop.
- Hepatocellular necrosis may result from direct toxic damage (e.g., acetaminophen) or a combination of toxicity and immune-mediated hepatocyte destruction (e.g., hepatitis virus infection).
- Rare causes of acute liver failure include abnormalities of blood flow, metabolic disorders, and malignancies (such as leukemia, lymphoma, breast cancer, and colon cancer)
- The etiology remains unknown in approximately 15% of adult cases and 50% of pediatric cases.
Check Medinaz Visual Mnemonic Books
Morphology
- Acute liver failure is characterized by massive hepatic necrosis, with regions of parenchymal loss surrounding islands of preserved or regenerating hepatocytes.
- The affected liver is small and shrunken in size.
- The extent of hepatocellular dropout and ductular reactions in the liver depends on the nature and duration of the insult. (ref)
- Toxic injuries, like acetaminophen overdoses, occur within a short period (hours to days), preventing scar formation or regeneration.
- Acute viral infections can lead to liver failure over weeks to a few months, where hepatocyte injury outpaces repair, but regeneration and scarring may be evident.
- Rarely, acute liver failure is associated with widespread dysfunction of liver cells without apparent cell death, such as in diffuse microvesicular steatosis related to fatty liver of pregnancy or idiosyncratic reactions to toxins (e.g., valproate, tetracycline).
- In these cases, hepatocyte metabolism is severely affected, often due to mitochondrial dysfunction, impeding the liver’s normal functions.
- Immunodeficiency states, like untreated HIV infection, posttransplant immunosuppression, and certain lymphoid malignancies, can result in acute liver failure caused by nonhepatotropic viruses, particularly cytomegalovirus, herpes simplex viruses, and adenovirus
- The incidence of these viral hepatitis forms is decreasing with improved HIV treatment.
Clinical Features
- Acute liver failure presents with nausea, vomiting, and jaundice initially, followed by life-threatening encephalopathy and coagulation defects.
- Markedly elevated serum liver transaminases are typical.
- The liver initially enlarges due to hepatocyte swelling, inflammatory infiltrates, and edema, but shrinks as parenchyma is destroyed.
- Decline in serum transaminases is not a sign of improvement but indicates few viable hepatocytes remaining, confirmed by worsening jaundice, coagulopathy, and encephalopathy.
- Unabated progression leads to multiorgan system failure and, without transplantation, death.
- Other manifestations of acute liver failure include:
Cholestasis:
Cholestasis, resulting in jaundice, icterus, and increased risk of bacterial infection.
Hepatic encephalopathy:
Hepatic encephalopathy with varying levels of consciousness disturbance, including subtle behavioral abnormalities, confusion, stupor, coma, and death. Associated fluctuating neurologic signs include rigidity and hyperreflexia
Coagulopathy:
Coagulopathy due to hepatic synthesis deficiency of clotting factors II (prothrombin), V, VII, IX, X, XI, XII, and fibrinogen, leading to easy bruisability and potentially fatal bleeding.
Portal hypertension:
Portal hypertension, seen less commonly in acute liver failure than in chronic liver failure, resulting in intrahepatic obstruction and ascites.
Hepatorenal syndrome:
- Hepatorenal syndrome, a form of renal failure occurring in individuals with liver failure without intrinsic kidney dysfunction, marked by decreased urine output and elevated blood urea and creatinine levels. It is triggered by portal hypertension and increased vasodilator production, leading to renal failure.
- The decline in renal function is reversible if liver function is restored, such as through liver transplantation.
- Hepatorenal syndrome can occur in the context of cirrhosis, severe alcoholic hepatitis, metastatic tumors, or fulminant hepatic failure from any cause.
Reference:
- Robbins & Cotran Pathologic Basis Of Disease; 10th Ed
- Visual Mnemonic Pathology; Dr. Nazmul Alam; 2nd Edition
- Text Book of Pathology; Dr. Harsh Mohan; 8th Edition
A Visual Learning Platform



